PLEASE VISIT OPENINGS FOR COMPENSATION INFORMATION ON VARIOUS PRACTICE OPPORTUNITIES
- Physiatry Compensation
- Compensation Formulas
- Questions to Ask and Issues To Consider When Evaluating Compensation Plans
Physiatrist (PM&R) Compensation Overview – 2024–2025
Sources: Medscape Physician Compensation Report 2025, Doximity Physician Compensation Report 2024; Physician Side Gigs; ZipRecruiter; MedScape; Marit
Average Annual Compensation for Physiatrists
On average, physiatrists (doctors specializing in physical medicine and rehabilitation also referred to as PM&R) make about $365,500 per year in clinical practice.
Physiatrist Salaries by State
PM&R pay varies a lot depending on location. In 29 states, the typical salary is above the national average. For example, Washington tops the list at about $273,000, while Florida is on the lower end at around $180,000.
| State | Annual Salary |
| Washington | $273,290 |
| District of Columbia | $272,670 |
| New York | $263,985 |
| Massachusetts | $263,524 |
| Alaska | $259,862 |
| Vermont | $256,558 |
| North Dakota | $255,310 |
| Oregon | $255,118 |
| Colorado | $253,726 |
| Hawaii | $250,696 |
| Nevada | $245,713 |
| New Jersey | $244,972 |
| Wisconsin | $243,552 |
| Pennsylvania | $241,875 |
| Delaware | $241,503 |
| South Dakota | $241,295 |
| Virginia | $239,226 |
| California | $238,136 |
| Minnesota | $236,328 |
| Rhode Island | $236,303 |
| New Hampshire | $234,662 |
| Maryland | $234,187 |
| New Mexico | $233,833 |
| Illinois | $233,821 |
| Maine | $233,622 |
| Wyoming | $231,938 |
| Nebraska | $230,063 |
| Indiana | $229,608 |
| Connecticut | $229,541 |
| Ohio | $229,399 |
| Mississippi | $228,523 |
| Idaho | $227,034 |
| Iowa | $226,640 |
| Missouri | $226,336 |
| Arizona | $224,860 |
| Texas | $224,804 |
| South Carolina | $223,911 |
| Oklahoma | $222,796 |
| Montana | $221,472 |
| Utah | $219,668 |
| North Carolina | $219,290 |
| Tennessee | $219,004 |
| Alabama | $218,707 |
| Kansas | $215,199 |
| Michigan | $210,312 |
| Kentucky | $209,572 |
| Louisiana | $206,338 |
| Georgia | $203,746 |
| Arkansas | $199,528 |
| West Virginia | $186,803 |
| Florida | $180,318 |
Salary by Employment Type
- Practice owners/partners: $482,000
- Employed/W2 physicians: $345,000
Salary by Gender
Female physiatrists reported average salaries of $329,000, while male physiatrists earned about $411,000 (25% more). Women were more likely to work in government or hospital jobs, while men often worked in private practices that tend to pay more.
Subspecialty Salaries
- Pain: $437,000
- Sports: $345,000
- Spinal Cord Injury (SCI): $291,500
Pain management is the highest-paying subspecialty in physical medicine and rehabilitation. On average, these doctors make $439,000 per year. Reported salaries range from $250,000 to $736,000, with a median of $400,000.
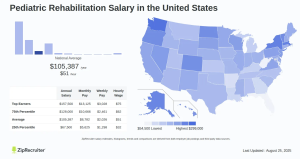
Pediatric Rehab
We identified 10 cities where Pediatric Rehabilitation salaries exceed the national average of $105,387. Nome, AK leads, with Cupertino, CA, and Nantucket, MA close behind. Nantucket surpasses the average by 23%, and Nome by 24%.
| City | Annual Salary |
| Nome, AK | $130,732 |
| Cupertino, CA | $130,020 |
| Nantucket, MA | $129,676 |
| Berkeley, CA | $129,040 |
| Sitka, AK | $126,957 |
| Sunnyvale, CA | $125,380 |
| San Francisco, CA | $124,164 |
| Santa Clara, CA | $123,770 |
| Livermore, CA | $123,617 |
| San Jose, CA | $123,512 |
Salary by Practice Setting
Where physiatrists work matters significantly for their pay; private practice physicians tend to earn the most, especially those who are owners or partners. Yet, it’s essential to consider the entire compensation package.
- Government hospitals (VA, city hospital, etc.): $274,000
- Academic hospitals: $296,000
- Non-academic hospitals: $434,000
- Private group practices (private equity and non-private equity backed): $454,000
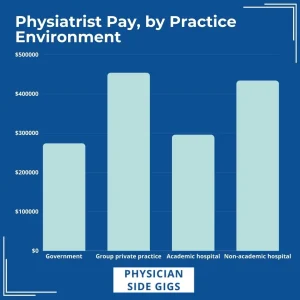
Overall, we see that PM&R doctors working in government facilities averaged the lowest salaries. They made 8% less than academic hospital employees, 58% less than those at non-academic hospitals, and 66% less than those at group private practices. It’s important to note, however, that these positions often qualify for Public Student Loan Forgiveness (PSLF) or have better retirement benefits, which can be a significant benefit in the overall compensation package, which is one of the reasons we suggest considering the entire proposed compensation offer.
Physiatrists at non-academic hospitals averaged 47% more than colleagues working for academic hospitals, but these positions often qualify for Public Student Loan Forgiveness (PSLF).
PM&R physicians working in group private practices averaged the highest salaries. Many of these reported being an owner or partner in their practice, which can influence potential earnings. We don’t currently have enough data to assess an average for physiatrists running a solo private practice, but generally, they make more than the average across all PM&R doctors.
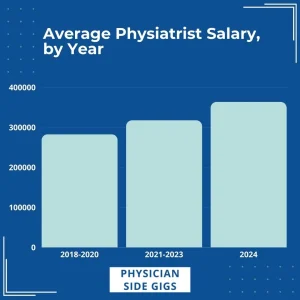
Salary Growth Over Time
Physiatrist pay has increased steadily over the last 7 years.
- 2018–2020: $283,000
- 2021–2023: $318,000 (+12%)
- 2024: $364,000 (+14%)
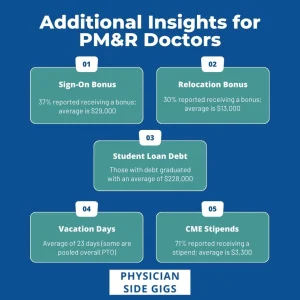
Bonuses
- Sign-on bonus: 37% receive one, averaging $29,000 (range $5k–$100k)
- Relocation bonus: 30% receive one, averaging $13,000 (range $5k–$60k)
Vacation
Most physiatrists receive between 21 and 23 days of vacation per year. Some report ‘unlimited’ time off, but usually only get paid for days worked.
CME Stipends
About 71% of physiatrists receive funding for continuing medical education (CME). The average stipend is $3,300 per year. (range $1k-$7.5k)
Student Loan Debt
The average student loan debt for physiatrists at graduation is $228,000. Government and academic hospital jobs may qualify for Public Service Loan Forgiveness (PSLF), which can help offset lower salaries. The higher your federal loan debt burden, the more beneficial repayment programs and loan forgiveness programs can be.
How to Increase Income
There are several ways to increase your income in PM&R. However, remember to look at the overall picture. Salary is a key component of physician compensation, but it isn’t the only part of a well-negotiated physician employment contract.
Ways to boost earnings include:
- Discuss your salary with your manager
- If you like where you work but don’t love the pay, consider setting aside a time to talk with management. If you are a valued part of their team, they may be willing to work with you to renegotiate your contract, rather than risk your leaving. Their answer may be no, but it doesn’t hurt to ask.
- Negotiating contracts
- Hire a local contract review attorney for physicians to review your contract. They will have invaluable experience when it comes to negotiating physician contracts, including understanding what red flags to watch out for.
- Changing practice setting
- Interviewing for a few other positions can give you a feel of what the market looks like from the employer’s perspective, and what employers are willing to offer.
- Taking on side work: 37% of physiatrists said they supplement their income with extra work
- Consulting, including consulting for pharmaceutical companies, and being a startup advisor
- Medical surveys
- Ambulatory surgery center owner
- Expert witness
- Running a pain clinic
- Offering concierge services
- Providing outpatient physician therapy/rehab services
How to Negotiate Your Physiatry Compensation
Negotiating your compensation as a physiatrist is an important step in setting yourself up for long-term career success. To do it well, you’ll want to prepare, practice, and protect your interests. Here’s a step-by-step approach:
Start with a plan
Make a list of your qualifications, skills, and accomplishments. This includes your training, board certifications, unique skills (like EMG or interventional spine), research, or leadership experience. Having this written out will help you confidently communicate your value.
Know your market value
Research what physiatrists with your background are earning.
- New residency graduates can typically expect anywhere from $175,000 – $300,000, depending on location, practice type, and demand.
- Use tools like the AAPM&R Salary Survey, MGMA benchmarks, or even conversations with colleagues to compare offers.
- When onsite, ask physicians with similar experience (confidentially and respectfully) what a reasonable compensation package might look like.
Practice your ask
Plan how you’ll phrase your request and how you’ll respond to pushback. Negotiating is expected — employers won’t see it as rude if you approach the conversation professionally. Remember: only the employer knows how high they can go.
Keep these tips in mind
- See it from their perspective: Highlight how you’ll add value to the practice (e.g., patient volume, procedures, teamwork).
- Look beyond base salary: Incentives, bonuses, relocation assistance, student loan repayment, and CME funding can be just as important.
- Understand compensation drivers: Productivity, quality measures, and cost management often affect bonuses.
- Secure a strong base: Negotiate for a base salary that would still be fair if you didn’t receive productivity bonuses.
Review the contract carefully
Before signing, make sure your contract spells out:
- Rounding responsibilities
- Clinic hours and office duties
- Patient volume expectations
- Average weekly workload
- Weekend and holiday coverage policies
- Clarity up front helps you avoid surprises later.
Bottom line: Negotiation is about advocating for your worth while building a strong, professional relationship with your employer. By doing your research, preparing your case, and carefully reviewing your contract, you’ll be in a much better position to secure fair and competitive compensation.
Compensation Considerations
These insights are from Kathy Jefferies, whose expertise stems from years of experience in physician relations at a hospital.
“One physiatrist expressed an interest in building a part-time practice performing only electromyography (EMG). That physician was obviously well informed about medical billing, and he desired to build a practice with only high-level billable codes. If you entered into practice with this physiatrist on a production-based compensation, what type of practice could you expect to build and how much money might you earn monthly? First, you need to determine the primary needs of the patient population in the practice area.
“As an employee, you will receive financial compensation based on a salary guarantee, production or a combination of both. A salary guarantee is an amount you can bank on, literally, and it may be a great way to start up your practice. However, no group will want to continue to pay you more than you earn. It just isn’t good business. That means it is expected that your gross charges will increase as your practice grows. Your earning potential will typically be production-based, or tied to the revenue you generate for your group. This is an important point to consider as you begin your contract negotiations.
“Production is typically not the best option for a start-up practice for several reasons. It takes an investment of time and money to build a practice, and this may be one of the most underestimated aspects of medical practice start-up. Retirement benefits within a group practice may exceed those available in hospital-owned practices — a notable advantage. Group practices tend to invest the maximum allowable amount — $30,000 annually — into each retirement plan for each physician in the group. In some groups, that money is self-directed, so each physician can elect their own investment options independently of the group. Hospitals, however, have a different set of governmental guidelines as not-for-profit or for-profit entities and are thereby limited in the amount that they can invest in the retirement plan for their employed physicians.
“In addition, there may be limited investment options for physicians in those plans. This is an important point to include in physician compensation when comparing practice opportunities and negotiating salary compensation. I have worked with many physicians who have built medical practices through trial and error. If some of these shared experiences help to shorten that course for you, I have met my goal.”
Physiatry Supervision Compensation
According to the American College of Physicians (ACP) Online, practices that employ nurse practitioners (NPs), physician assistants (PAs), or other non-physician providers may require some oversight time. In practices that use production-based compensation models, such as Work Relative Value Units (wRVUs), this oversight can present challenges because the time spent on supervision is considered non-productive, even though it is essential for the effective operation of the practice.
To address this, compensation structures can be designed to include a production credit or a supervisory stipend. Ultimately, it is crucial to ensure that any compensation formula results in fair total compensation that falls within the fair market value range.
Compensation With an Independent Contractor Affiliation
Some practice opportunities don’t offer a salary because the affiliation is as an independent contractor. Companies such as Encompass and Kindred typically affiliate with a physiatrist as an independent contractor. They offer a stipend for the Medical Director position. The stipend varies based on the bed size, the reasonable and fair compensation for physiatry in the area, and more. Medical Director stipends can range from $60,000 – $120,000.
An income guarantee may also be offered when it’s an independent contractor affiliation. The guarantee amount is comparable to the salary that would be expected for the same position. The guarantee is typically a loan with repayment terms. In these arrangements, failing to meet your guarantee amount results in having to repay the difference, which is a significant drawback when it occurs. However, most of these cases involve large rehabilitation institutions with a good census, so there’s usually no concern that you wouldn’t meet your guarantee amount and would have to reimburse them.
Medical Director Compensation
The average Medical Director Stipend for a 15-bed rehab unit varies from facility to facility. It depends on the individual facility and its specific needs and expectations. The exact amount the Director receives is based on a predetermined hourly fee for administrative costs only. The contract usually stipulates a mandatory 20 hours per week of administrative time. The facility typically generates a form for the Medical Director to use to document their time. The average hourly rate is from $100 to $150 per hour.
When negotiating the contract for the per-hour rate, the physician must be aware of what encompasses the administrative time. The easiest way to determine this is to ask to see their reporting form. This should list each of the categories that you would spend administrative time on.
(Contributed by Elizabeth Lee, PRS, Former President)
Questions to Ask & Issues to Consider When Evaluating Compensation Plans
Determine how the compensation plan works, initially and at different points in time. It is perfectly reasonable for a physician to ask how much he or she will be paid in the first year and in subsequent years. For example, if the first one or two years’ salaries are fixed, and compensation then moves to a productivity basis, ask for details on how the transition is handled and how other physicians have fared in year two or three. The bottom line, Merritt Hawkins EVP Mark Smith says, is that “if physicians can’t determine how much they will earn while they’re brushing their teeth, the (plan) is too complex.”
Inquire about how overhead expenses are allocated. In most cases, newly hired physicians will receive a “grace period” in the first year from financial responsibility for overhead. But those expenses, which could equal up to half of a group’s revenues, may be a significant consideration when the physician becomes a partner or shareholder. “Physicians should ask whether there are any limitations based on overhead,” Smith advises. “For example, if there’s a net income guarantee of $175,000 and only $5,000 monthly is allowed for overhead, that won’t work well.”
What is the income distribution methodology for partners or stockholders? Even if the position will be a straight salary initially, physicians should inquire about how income is distributed among the group’s partners and which factors, if any, affect the proportional distribution among individual physicians.
What is the buy-in and how does it work? Since many practice positions involve either net income guarantees or salaries in the early years, entrepreneurial physicians who desire an ownership position should request the details if they’re considering more than one position. A five-year partnership track may be less appealing than a two-year track, for example, and the longer route to partnership may result in lower long-term earning potential.
For the complete article, “Physician Compensation Models: The Basics, the Pros, and the Cons,”
Compensation Formulas
Practices, hospitals, and other entities compensate physicians in many ways. Multiple variations of these formulas are possible, so your task is to identify the combination that works best for you. As a physician reviewing the compensation formula that involves collections or office expenses, you need to get a handle on what these items realistically might total.
Partnership Potential
Partnership is one of the important things for physiatrists to consider, as it has a significant impact on PM&R compensation. Here are six formulas you might encounter for determining compensation along partnership tracks.
For these calculations, expenses typically include professional physician expenses and administrative expenses for the entire group. Professional physician expenses include the base salary, the cost of health and malpractice insurances and the cost of professional society dues, journal subscriptions and other professional fees. Administrative expenses of the practice include all items not included in professional physician expenses, such as rent, utilities, employees’ salaries and benefits, marketing and advertising, legal and accounting expenses and equipment purchase or lease payments.
Salary Plus Incentive
Compensation with this type of plan is typically a $175,000 – $185,000 salary plus an incentive. Incentive plans are often 20% of collections on physician-provided services after three times the salary. For example, a salary of $180,000 with collections of $600,000 would result in a $12,000 incentive bonus:
- $180,000 x 3 = $540,000
- $600,000 – $540,000 x 20% = $12,000
Salary Then Production
Another option is straight salary without incentives for the first two years, then a transition to compensation based 100% on your production.
Salary to Partnership
This track typically starts with a base salary of $250,000 with 10% share after expenses for the first year. The second year, the salary increases by $20,000 with a 15% share of expenses, and the third year is a partnership.
Salary Plus Incentive to Partnership
A formula like this is a little more complicated. The salary is usually between $160,000 and $175,000 plus an incentive, which changes each year. The first-year incentive formula is 20% of the difference between the net income minus expenses. The second year, the incentive is 30% of that difference, and the third-year incentive is 40%. The fourth year transitions to a partnership.
Salary Plus Bonus
This is similar to the incentive model, but the bonus is calculated differently. Since there is potential for a higher bonus, the base salary is a little lower, typically around $150,000. The bonus has no limit and is based on productivity and length of service. The bonus is calculated as a percentage of “net” revenue, once general practice overhead and physician expenses — including base salary — are deducted. The percentage is 40, 45 and 50% in the first, second and third years, respectively. Net earnings are defined as gross earnings minus professional physician expenses and 50% of the practice administrative expenses.
Partnership will be considered after two or three years in practice.
An example sometimes helps. This is all very hypothetical, and numbers are only used that make for easy calculations:
- Gross collections for the quarter: $150,000
- Overhead expenses: $60,000
- Physician expenses: $60,000
- Net: $30,000
- Bonus at 40%: $12,000 for the quarter
Draw Plus Stipend Plus Productivity Bonus
You can set the draw up to $250,000. The physician plan allocates overhead in two ways. Part of the overhead — usually 20% — is distributed equally, and the rest is allocated based on receipts. Thus all physician partners have a basic share of the overhead, and those who produce more revenue and consume more resources are allocated a greater share for the rest of the overhead.
New physicians are paid the draw until their practice grows to the point that receipts cover the incremental costs incurred by adding the new doctor.
Employee Affiliation
There are three main types of compensation possible for employee affiliation.
1. Income Guarantee Plus Incentive
This is typically an income guarantee of $200,000 and incentive of 33% of production after overhead is covered.
2. Income Guarantee With Possible Incentive
Because the potential incentive is higher with this method, the income guarantee is lower, usually between $160,000 and $180,000. If a straight percentage method pays more than the salary, then the candidate can switch over to it before the first year.
The incentive will be available if the candidate makes two times their income guarantee. The incentive formula is net income minus two times the salary. The doctor gets 50%, and the other 50% goes to cover overhead.
For example, if the net income is $400,000 and the income guarantee is $150,000, then the incentive payment is $50,000:
- $150,000 x 2 = $300,000
- $400,000 – $300,000 = $100,000
- $100,000 x 50% = $ 50,000
A similar method is with a guaranteed salary of $120,000 to $135,000 plus an incentive which is 30% of triple the salary.
3. Salary Plus Bonus
This method offers a higher salary of $195,000 to $205,000 along with the potential to earn two separate bonuses. One is up to 10% of their salary, and the other bonus is 35% of their gross billings above their business plan.
Beyond Salary: Understanding PM&R Compensation and Benefits
When evaluating a physiatry job offer, compensation is often the first thing physicians focus on. Salary matters — but the total package is what really determines your financial well-being. Benefits, location, and taxes can dramatically impact your take-home pay and long-term financial outlook.
Benefits: The Hidden Value
Benefits are costly for employers to provide and can add significant value to your offer. Common examples include:
- Health insurance – usually provided, and very expensive to purchase on your own.
- Retirement plan contributions – some practices match a percentage of your contributions.
- Sign-on bonuses – a useful upfront perk, though often tied to a repayment clause if you leave early.
- Relocation assistance or loan repayment – less common, but negotiable.
Tip: Always ask whether you’ll have to pay back sign-on bonuses, relocation funds, or loan repayment assistance if you leave before a certain date. If you want flexibility, these incentives may not be ideal.
Compare Offers Side by Side
Sometimes, a position with a lower salary but strong benefits can outpace an offer with higher base pay. Employers are often willing to share the costs of the benefits they provide — ask for this information. Create a spreadsheet that tallies:
- Base salary
- Value of health insurance
- Retirement match
- Bonuses and incentives
The Cost of Living Factor
Compensation should always be weighed against the cost of living in the location.
- Big cities often pay less relative to expenses.
- Housing, commuting, meals, and entertainment can vary widely.
- A shorter commute saves both time and money.
- Use tools like Best Places’ Cost of Living Calculator to make direct comparisons between cities.
Taxes: The Overlooked Cost
State income taxes can eat away at your earnings — sometimes by millions of dollars over a career.
- States with no income tax: Alaska, Florida, South Dakota, Tennessee, Texas, Washington, Wyoming.
- High-tax states like California and Oregon can take 9% or more in state income tax.
Example: If you avoided California’s $17,227 annual state tax by working in Nevada and invested that money at 5% yearly growth:
- 10 years: $255,574
- 20 years: $643,817
- 30 years: $1,276,223
That’s the power of factoring taxes into your decision.
Bottom Line: When reviewing a physiatry job offer, look beyond the base salary. Weigh benefits, cost of living, commute, and state tax policy. The right opportunity balances all of these factors to support both your career satisfaction and long-term financial health.
If Doctors Chose Their Job Locations Based on State Income Taxes
Physiatry Reimbursement Rates Across Geographic Areas
Physiatrists often ask, “In which city or state would I earn the highest income?”
Medicare and other insurance carriers have different reimbursement rates depending on geographic locality, which in turn is based on factors such as practice costs like overhead and malpractice insurance. The most highly reimbursed areas are in the big cities and nearby suburbs. New York City reimburses more than Los Angeles, which in turn reimburses more than Houston.
Is the variation among localities significant?
Not as much as you may think. An analysis of I/P admission code 99223 shows that the National Average Medicare Allowed amount is $195. However, of the 90 localities in the country, 72 are within 6% of the national average! Only one locality is more than 6% below the national average — Puerto Rico. And only eight localities are more than 10% above the national average, including those you would expect:
- San Francisco, Anaheim and the surrounding areas
- Manhattan, Queens, Long Island and other New York cities
- Miami
If you want to locate your practice in a highly-reimbursed location, bear in mind that there is a tradeoff. Although you will be reimbursed more, the cost of running your practice will be higher, and in all probability, your personal living expenses will also be higher.
Here is a recommendation: start with an area you could see yourself enjoying, and then look at the numbers because by far, the most important determinant of practice income is the quantity of procedures performed – not the reimbursement.
But if you are looking at numbers only, the most highly-reimbursed area of the country for an I/P admission is Alaska – a full 33% higher than the national average. So, by the numbers, Alaska is the place to be — just remember to pack your thermal underwear and sled dogs.
Contributed by Bruno Stillo, Physiatry Billing Specialists
Back to Top
Find the Position You Deserve With Farr Healthcare
Farr Healthcare is the leading partner for physiatrists looking to begin their careers or find a new job. We have more than 30 years of experience recruiting physicians, and we make the process as simple as possible so you can find the right position based on your skills and experience. To get started, view our listed openings or fill out our physician application.







